What is a Hernia?
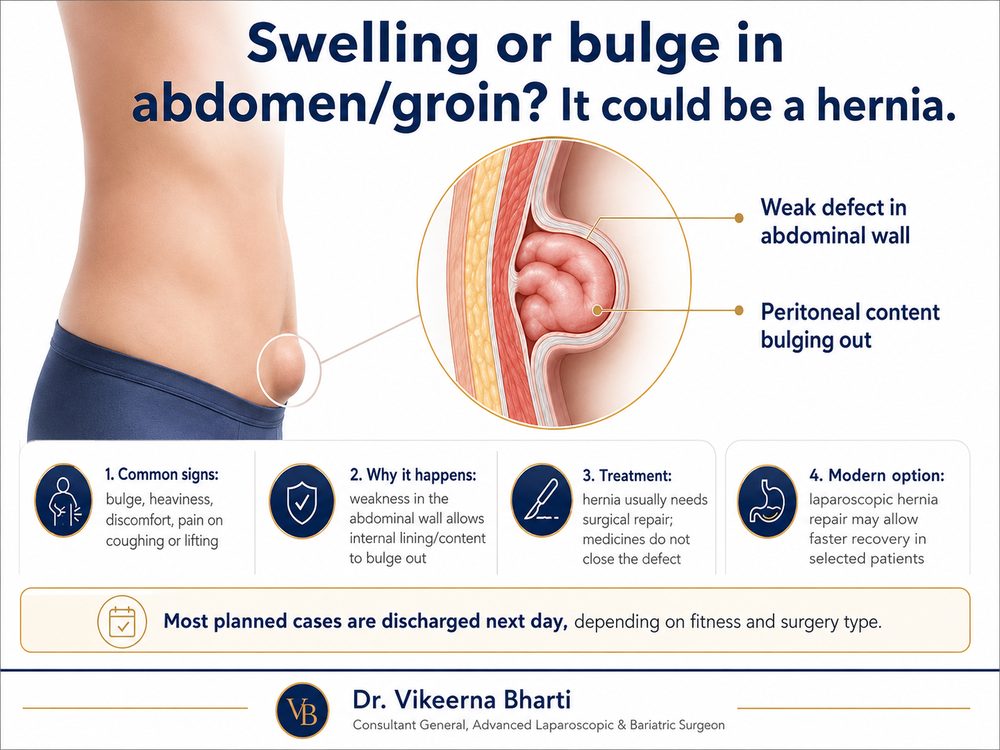
A hernia is a mechanical defect in the abdominal wall. It occurs when a weak spot or tear in the muscular layers allows internal abdominal contents — such as a loop of intestine or intra-abdominal fat — to protrude outward, creating a visible bulge beneath the skin.
Hernias do not improve or heal with medications, belts, or exercise. Left untreated, the muscle gap tends to enlarge under abdominal pressure. The primary risk is hernia incarceration or strangulation, where a section of the bowel gets trapped and its blood supply is cut off, which is a life-threatening surgical emergency.
हर्निया (Hernia) का रांची में स्थायी इलाज
हर्निया पेट की मांसपेशियों की दीवार में एक शारीरिक छेद या कमजोरी है, जो केवल ऑपरेशन द्वारा ही ठीक हो सकती है। दवाइयों से इसका कोई इलाज संभव नहीं है। डॉ. विकीर्ण भारती रांची के सैमफोर्ड अस्पताल में दूरबीन (लेप्रोस्कोपी) द्वारा हर्निया का सफल ऑपरेशन (TEP/TAPP/eTEP) करते हैं और जाली (Mesh) लगाते हैं। छोटे सुराख होने के कारण दर्द बहुत कम होता है और अधिकतर मामलों में अगले दिन अस्पताल से छुट्टी (next-day discharge) मिल जाती है। संपर्क करें: +91 62060 91982
Types of Hernias and Their Locations
Hernias are classified according to their location on the abdominal wall:
- Inguinal Hernia: Located in the groin. Most common in men; often presents as a groin bulge that expands when standing or straining.
- Femoral Hernia: Protrudes in the upper thigh just below the groin crease. More common in women and carries a high risk of entrapment.
- Umbilical Hernia: Protrudes through the natural weak spot around the belly button. Common after pregnancy or in overweight individuals.
- Ventral or Epigastric Hernia: Develops in the midline of the abdomen between the breastbone and the navel.
- Incisional Hernia: Develops at the site of a previous surgical incision due to healing failure of the abdominal muscle layers.
- Recurrent Hernia: A hernia that returns at a site previously operated on.
Symptoms and Indicators
Common clinical signs of a hernia include:
- A visible lump or bulge in the groin, belly button, or near a surgical scar.
- A bulge that expands or becomes hard when standing, coughing, or lifting objects, and disappears when lying flat.
- A dull ache, pressure, or dragging sensation around the bulge, especially at the end of the day or after physical strain.
⚠️ Emergency Symptoms of Strangulation:
- The hernia bulge becomes extremely painful, firm, or changes color (red/purple).
- The bulge cannot be gently pushed back into the abdomen while lying flat.
- Onset of vomiting, severe abdominal distension, and inability to pass gas or stool.
- These indicate a surgical emergency. Call +916206091982 or proceed directly to an emergency department.
Advanced Laparoscopic Repairs & AWR in Ranchi
Dr. Vikeerna Bharti utilizes advanced keyhole laparoscopic techniques to repair hernias, choosing the optimal method for each patient's anatomy:
1. Laparoscopic TEP and TAPP Repairs
For groin (inguinal) hernias, these methods utilize 3 tiny keyholes to work behind the abdominal wall. The hernia sac is reduced, and a high-strength anatomical mesh is placed to cover the entire weak zone. By placing the mesh behind the defect, abdominal pressure naturally pushes the mesh flat, creating a durable repair with minimal pain.
2. The eTEP Approach
The **extended Totally Extraperitoneal (eTEP)** technique is a significant advancement in hernia surgery. It allows the surgeon to access the retromuscular space of the abdominal wall without entering the peritoneal cavity where the intestines lie. This allows the placement of very large meshes to reinforce wide defects (such as incisional hernias) without placing mesh in direct contact with bowel loops, significantly reducing post-operative complications.
3. Abdominal Wall Reconstruction (AWR) & TAR
For complex, very large, or recurrent incisional hernias, simple mesh placement is associated with high failure rates. Dr. Bharti performs advanced **Abdominal Wall Reconstruction (AWR)**, including **Transversus Abdominis Release (TAR)**. This involves separating the muscle layers of the abdominal wall, allowing the surgeon to close the central defect naturally and place a giant reinforcing mesh in the retromuscular space. This restores the functional strength of the abdominal core, providing durable surgical relief in properly selected patients.
Recovery Timeline & Post-Operative Care
Laparoscopic repairs facilitate faster recovery and early mobilisation:
- Hospital Stay: Most planned laparoscopic hernia repairs are discharged the next day.
- Mobilisation: Walking is initiated on the same evening. Patients can climb stairs and do light chores within 48 hours.
- Returning to Work: Desk-bound office work can be resumed within 5 to 7 days.
- Lifting Restrictions: Avoid lifting weights over 5 kg and strenuous abdominal exercise for 4 to 6 weeks to allow full mesh integration.
Frequently Asked Questions
Yes, a bulge in the groin that appears on standing, straining, or coughing, and disappears when lying flat is typically an inguinal hernia. Hernias are defects in the abdominal wall and do not heal on their own; surgery is needed to repair the defect.
Laparoscopic hernia repairs typically take between 45 to 90 minutes. Most planned cases are discharged the next day. Patients can return to light activity in 5 to 7 days.
Laparoscopic (keyhole) hernia repair offers significant advantages, including smaller incisions, reduced post-operative pain, faster recovery, and a quicker return to normal activities. However, for extremely large or complex recurrent hernias, open Abdominal Wall Reconstruction (AWR) may be recommended.
The recurrence rate for modern hernia surgery using a high-quality mesh is very low, typically between 1% and 3%. Using proper surgical techniques and following post-operative guidelines (avoiding heavy lifting) reduces this risk further.
Umbilical hernia repair closes the muscle defect around the belly button. It can be performed laparoscopically or openly, and a surgical mesh is placed to reinforce the repair, depending on the size of the defect.
AWR is an advanced surgical technique used for large, complex, or recurrent abdominal wall hernias. It involves separating and moving the muscle layers of the abdomen to close the gap naturally before placing a reinforcing mesh.
Transversus Abdominis Release (TAR) is a type of component separation. It releases the innermost abdominal muscle layer to create extra space and allow closure of large defects without tension, reducing long-term recurrence rates.
You should consult a surgeon as soon as you notice an abdominal bulge. Early evaluation prevents complications like hernia incarceration or strangulation, which require emergency surgery.